Reinhardt tackles the question of explaining high US health care costs--that is, per capita US spending on health care is roughly double the average for other high-income countries. Here's a flavor of Reinhardt's take on four possible explanations.
Possible explanation #1: US income levels are higher, and health care spending tends to rise as incomes rise. Reinhardt writes:
Possible explanation #3: Health care, or at least certain kinds of health care, cost more in the US. Reinhardt writes:
Possible explanation #1: US income levels are higher, and health care spending tends to rise as incomes rise. Reinhardt writes:
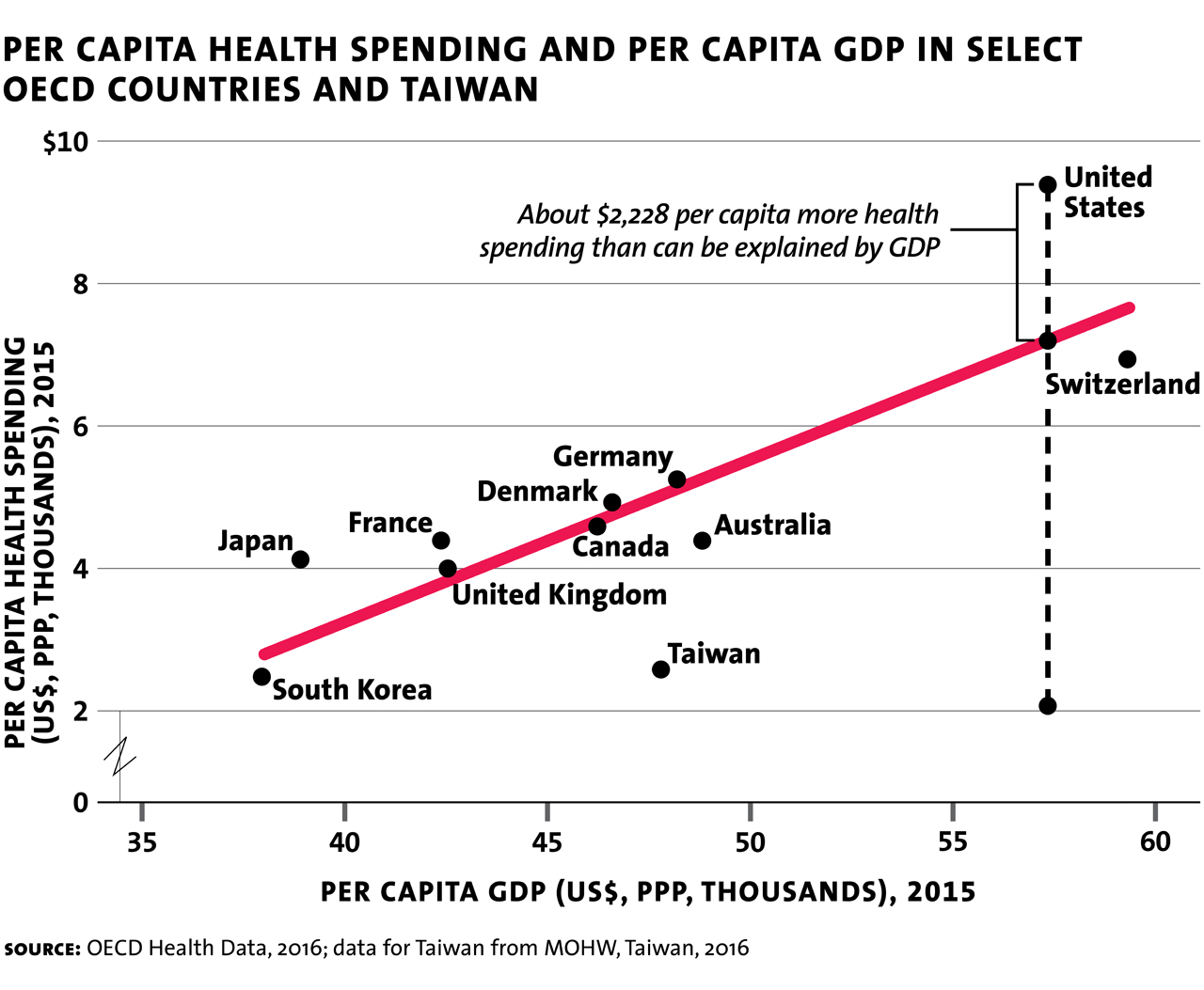
The figure shows that GDP per capita does indeed drive health spending systematically. But income alone leaves much unexplained. Even after adjusting the health spending data for GDP per capita (roughly, “ability to pay”), U.S. spending levels are much higher (about $2,200 higher in 2015) than would be predicted by the graph ...Possible explanation #2: US Demography leads to higher health care spending. Reinhardt writes:
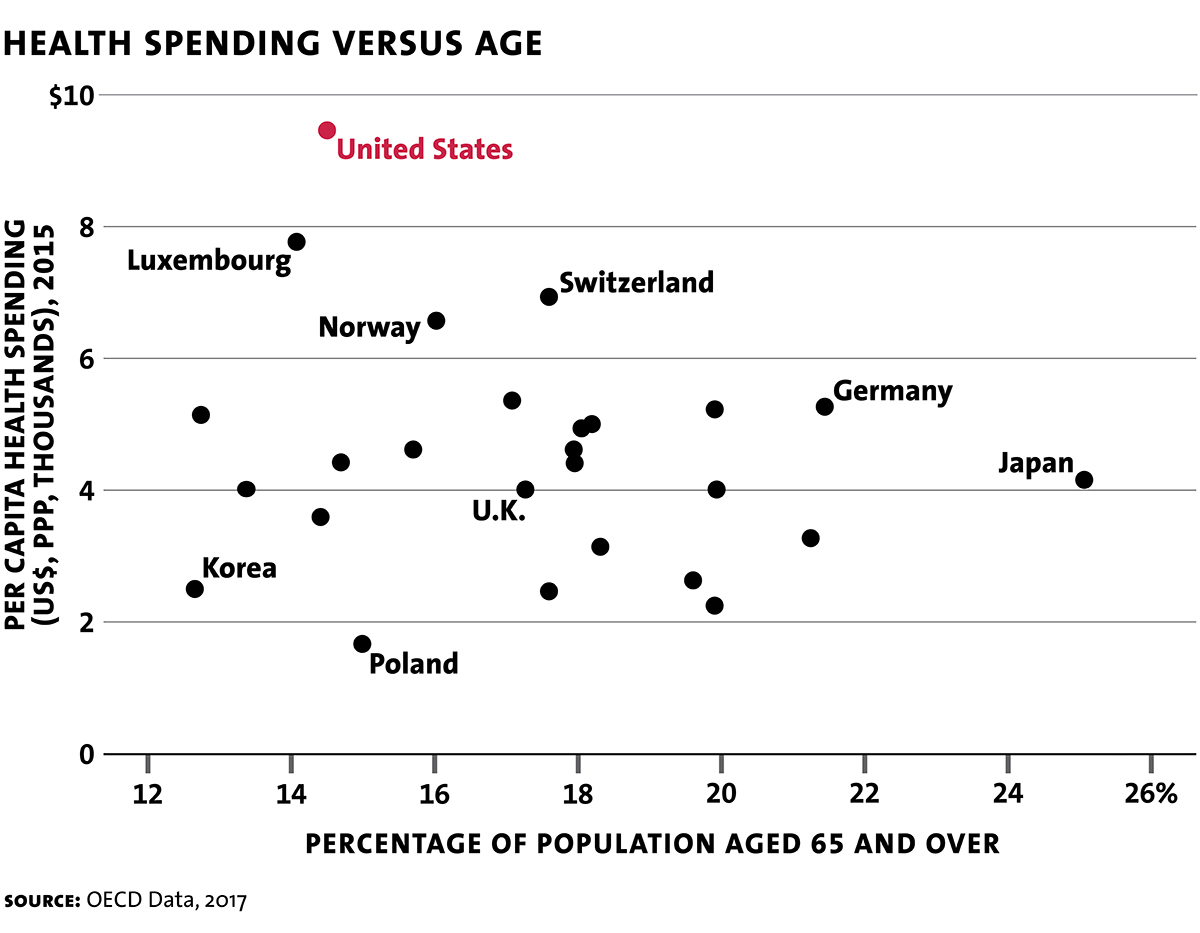
The U.S. population is, on average, much younger than the populations of most countries in the OECD, yet we spend much more per capita on health care. In fact, although the United States has one of the youngest populations among developed nations, we have (as noted earlier) the world’s highest health spending per capita. Japan, in contrast, has the oldest population, but among the lowest health spending levels.
Possible explanation #3: Health care, or at least certain kinds of health care, cost more in the US. Reinhardt writes:
With the exception of a few high-tech procedures, Americans actually consume less health care service in real terms (visits with physicians, hospital admissions and hospital days per admission, medications and so on) than do Europeans. For better or for worse — better for the vendors of health care and worse for consumers — prices for virtually every health care product and service in the United States tend to be twice as high as those for comparable products or services in other countries.Here are some examples of that pattern, using data from an International Federation of Health Plans report.
Possible explanation #4: High administrative costs in the US health insurance system. Here's Reinhardt:



According to a recent publication by America’s Health Insurance Plans, private health insurers on average take a haircut of about 17.8 percent off the insurance premiums paid by employers or individuals for “operating costs,” which means marketing and administration. Another 2.7 percent is profits. That haircut was as high as 45 percent pre-Obamacare for smaller insurers selling policies in the (non-group) market for individually purchased insurance. Under Obamacare the portion of the premium going to marketing, administration and profits was constrained to 20 percent for small insurers and to 15 percent for large insurers. ... It’s worth noting that some analysts of administrative costs of Blue Cross Blue Shield plans and other private insurers report that the AHIP number is too high. They currently estimate the range to be between about 9 percent for the Blues and between 10 and 11 percent for other private insurers. ...
Drugs that cost $17 to produce end up costing patients or purchasers of health insurance $100. Of a total $100 in consumer spending, health insurers pay pharmacy benefit managers $81, keeping $19 for themselves, of which $3 is profit. The rest goes for marketing and administration. ...
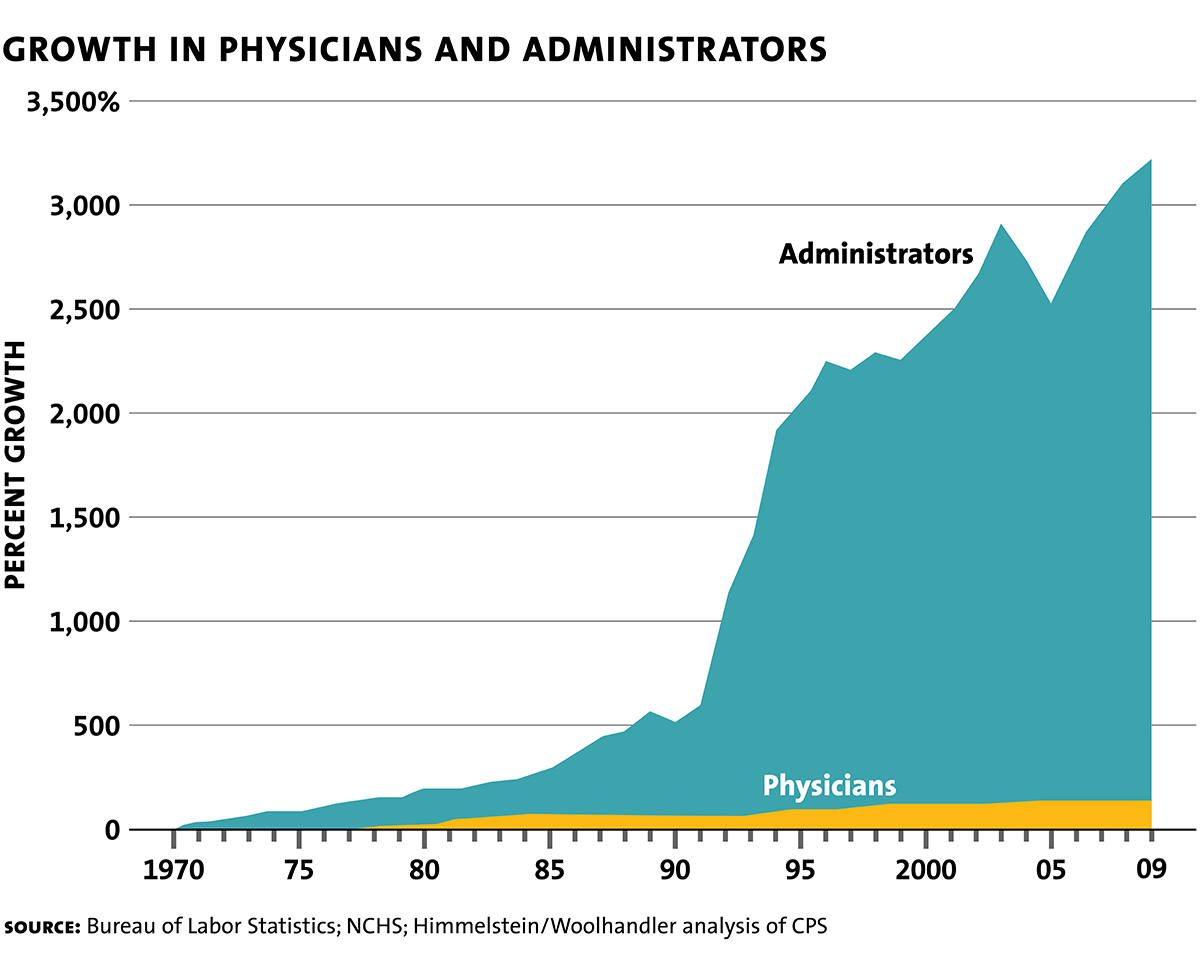
I can think of no legislation ever to emerge from Congress that addressed the magnitude of this administrative overhead. It is as if Congress just does not care what health spending actually buys. On the contrary, every health reform emerging from Congress vastly complicates the system further and brings forth new fleets of non-clinical consultants who make a good living teaching clinicians and hospitals how to cope with the new onslaught. All of their income becomes the providers’ expense and thus ends up in the patient’s bill.And here's one more figure from Reinhardt, showing the growth in health care administrators vs. the growth in actual health care providers over time.
Of course, this post is only an appetizer. There's much more in the MIR article, and much much more in the book itself.